Measles outbreaks in late 2024 and early 2025 have reignited media-driven panic. Infectious disease experts are back in the spotlight, warning of a public health crisis. Are we losing control of measles? Is vaccine coverage across the world irreversibly trending away from public health goals? How terrified should we be?
The requests for interviews have likely spurred a lot of discussions on how to handle the measles “situation”. Public health spokespeople are thrilled to be able to reach, at last, thousands of people about what they suggest is an insidious, progressive, and significant public health crisis.
This intense focus has been fuelled by a public health campaign that delivers a straightforward, who-in-their-right-mind-could-possibly-disagree-with-it message: measles is a serious disease, its return is an emergency, every child is at risk of complications, the MMR shot is virtually risk free, and vaccination saves lives. To an innocent consumer of mainstream media, any reported decrease in measles vaccine uptake amongst children aged 2 years borders on the unethical.
Even media articles outside the mainstream – including on this platform – echo claims that measles is a terrible disease with serious side effects, hurting mostly children.[1]
The historical narratives surrounding measles and measles vaccine programs are complicated and require subtlety in public discussion. When people say things like, “were it not for childhood vaccinations … childhood death rates would probably hover in the range of 20 to 50%”[2], they are speaking beyond what they know.
There is another communication problem. Through the media, public health tends to approach the future by depicting what can happen as what will happen. Rare complications of many vaccine-preventable diseases are presented as the rule rather than the exception.
If 1 in 1,000 (0.1%) detected measles cases experience encephalitis, the crucial message – that 99.9% measles cases do not – goes unsaid. Instead, there is an implicit warning to parents: vaccinate to avoid being that one case. Such is the standard public health formula: cater to scary things; promote a solution; repeat.
If people can be convinced that measles is a real public health priority, then governments can justify big initiatives and enormous expenditures that are independent of their usefulness or sustainability.
There are some of us in the world of epidemiology who are thinking hard in this time of opportunity about how to boil down what needs to be said, and how to say it with the right degree of certainty. Here, after many months of scary measles tales, is the best I can do:
We know that measles (the virus, not the disease) spreads easily through the air when an infected person coughs or sneezes. In epidemiology, the ease with which spread occurs is sometimes described by the basic reproductive number (R0, pronounced “R nought”).[3] For measles, R0 is typically thought to range from 12 to 18, making it one of the most easily transmitted infections.
However, R0 is mostly estimated with various types of complex mathematical models, which makes it an easily misrepresented, misinterpreted, and misapplied concept.[4] The oft-quoted values of R0 for measles are based on – dare I say, outdated – data from 1912–28 in the United States and 1944–79 in England and Wales.
Despite its high value for measles, R0 cannot tell us how large, or how severe, an outbreak or epidemic will be. Even outbreaks with high R0 values can vanish before any immunity accumulates or any interventions are introduced – a phenomenon called “epidemic fadeout”.
We know that – despite measles’ formidable reputation – most cases are benign with many (upwards of 90%) going unreported to public health agencies such as the CDC.[5] [6]
Before mass vaccination programs, it was rare for a child to suffer permanent disability or death. In the 1960s, even strong advocates for measles eradication described measles as a “short, moderately severe, self-limiting infection with low fatality rates.” Targeting measles for global public health action was “because it is there” rather than because of its total disability days or number of deaths.[7]Children faced greater risks from other causes (Figure 1).
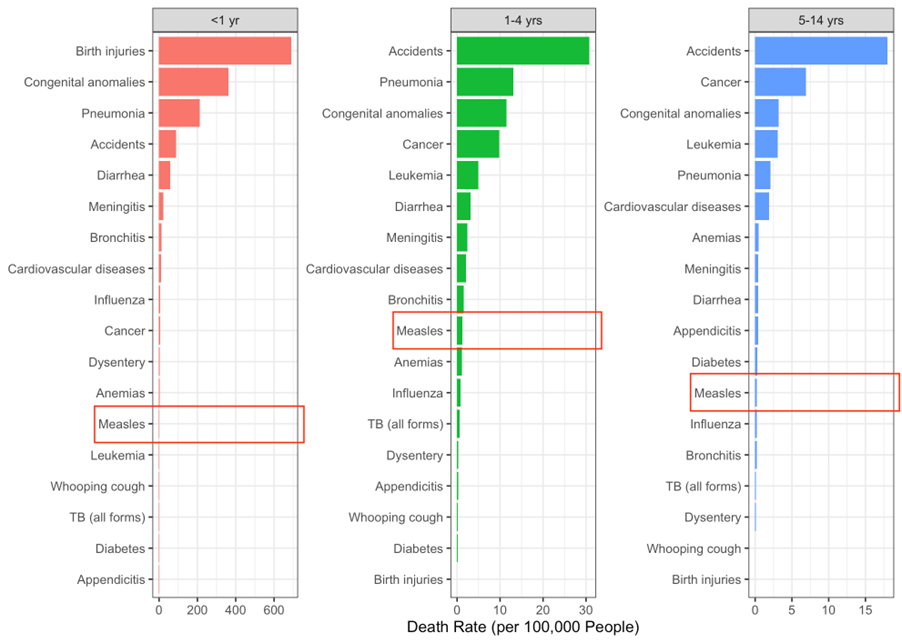
Figure 1 – Death rates from 18 causes in U.S. children (<1, 1–4, and 5–14 years) in 1962, the year before measles vaccines were first licensed for public use. Note the different x-axis scales. Data from CDC’s National Vital Statistics System.[8][9][10][11]
We know that from 1940 to 1962, measles mortality in U.S. children dropped 88–92% before vaccine programs began in 1963 (Figure 2). This decline – largely due to better food, safer water, cleaner air, and improved sewage disposal – continued without clear evidence that vaccine programs accelerated it.
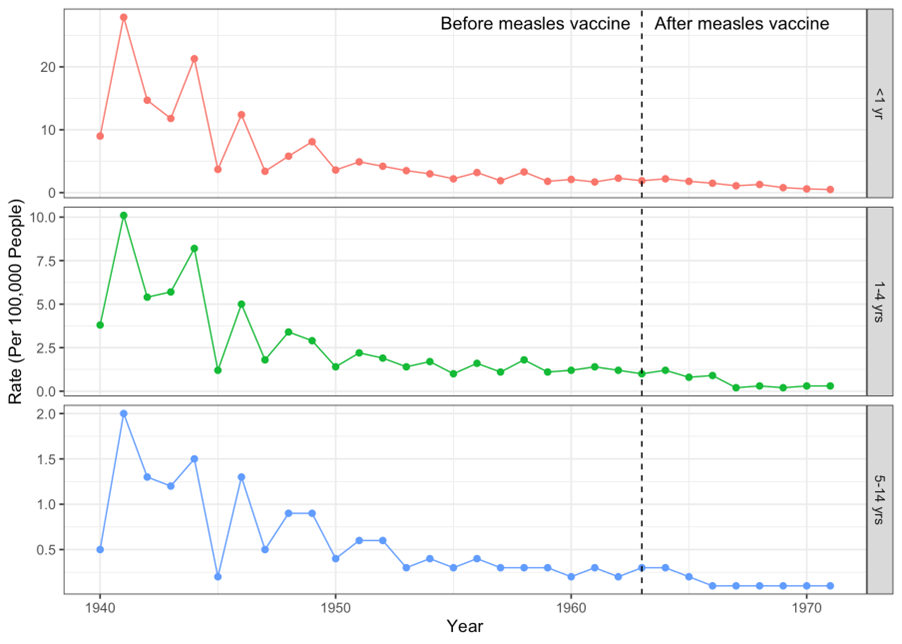
Figure 2 – Age-specific measles death rates in U.S. children declined 88-92% from 1940 to 1962. Measles vaccines were introduced to the public in 1963 (vertical dashed line). Note different y-axis scales. Data sources are the same as Figure 1.
We know that, despite being rare, measles (the disease) can be serious for some people, and there are complications that can arise including: seizures, middle-ear and lung infections, brain swelling, hospitalization, and death.
However, we also know that malnutrition, especially vitamin A deficiency, is a major driver of measles mortality in young children in underdeveloped countries,[12]because it diminishes their ability to fight infection. In developed countries, 75-92% of hospitalized measles patients are low in vitamin A.[13][14]
Severe neurological outcomes including encephalitis or subacute sclerosing panencephalitis (SSPE) have little to do with an active measles infection,[15]and are likely tied to pre-existing immune dysregulation.
We know that infants born to mothers with natural immunity have longer protection than those born to vaccinated mothers.[16]
We know that measles vaccine programs have significantly reduced the number of reported cases since beginning in the early 1960s. For many in public health, this is the only relevant marker – from this point on, progress has been indefinite, and there will be no point at which the benefits of vaccine programs will stop.
However, to the surprise of many, a counter-productivity has set in, and national programs are no longer working according to plan. Their emphasis on “how many are vaccinated” vs. “whom” is a contrived, one-size-fits-all solution that is having wide-ranging, unanticipated consequences. Everyone can act dutifully and rationally, and these well-meaning actions can still lead to an undesirable result.[17]
The self-maintaining capacity for high levels of immunity that happened before large-scale vaccination has been eroded,[18]and an unwanted consequence has been set in motion: slowly, over time, population-level immunity from natural re-exposure deteriorates; population-level immunity is increasingly dependent on vaccination, and many nations are unable to maintain “measles elimination” status. Measles vaccination programs have become victims of their own success.
The vaccine era has turned a once-common, manageable illness into a threat. For many, however, this is easy to overlook since threats are so often conflated with real dangers. Improved living conditions nearly purged measles deaths decades ago. The “return” of measles is not an emergency but a predictable outcome of current strategies. The promise of eradication by 1967[19]remains unfulfilled, distorted by an emphasis on fear.
Notes & References
[1] Hunt L. Accountability and Measles Outbreaks. BIG Media, June 20, 2025
[2] Sherman I. Twelve Diseases that Changed Our World. Wiley Publishing, 2007: page 66
[3] R0 must be estimated, reported, and applied with great caution because this basic metric is far from simple. R0 is affected by numerous biological, social, behavioural, and environmental factors that govern pathogen transmission. R0 is rarely—if ever—measured directly
[4] Delamater PL, et al. Complexity of the Basic Reproductive Number (R0). Emerging Infectious Diseases 2019; 25(1): 1-4
[5] CDC. Epidemiology and Prevention of Vaccine-preventable Diseases. 13th ed. Hamborsky J, Kroger A, Wolfe S, editors. Washington, DC: Public Health Foundation; 2015. Appendix E3
[6] CDC. Measles Prevention: Recommendations of the Immunization Practices Advisory Committee (ACIP). MMWR, 1989; Dec 38(S-9):1
[7] Langmuir AD et al. The Importance of Measles as a Health Problem. Am J Public Health, 1962: 52(2); 1–4
[8] Yang HM, et al. Vitamin A for Treating Measles in Children. Cochrane Database of Systematic Reviews 2005, Issue 4. Article: CD001479
[9] CDC. National Vital Statistics System, Unpublished trend table, and Vital Statistics of the United States (1950-1959)
[10] CDC. National Vital Statistics System, Mortality, Unpublished trend table 290A for 1960-67 and separate unpublished tables for the black population and Accidents
[11] CDC. National Vital Statistics System, Mortality, Unpublished trend table 290 for 1968-78
[12] Yang HM, et al. Vitamin A for Treating Measles in Children. Cochrane Database of Systematic Reviews 2005, Issue 4. Article: CD001479
[13] Butler JC, et al. Measles Severity and Serum Retinol (Vitamin A) Concentration among Children in the United States. Pediatrics, 1993 Jun 91(6): 1177-1181
[14] Hussey GD, Klein M. A Randomized, Controlled Trial of Vitamin A in Children with Severe Measles. N Engl J Med 1990 Jul 19; 323(3): 160-164
[15] Garg RK. Subacute sclerosing panencephalitis. Postgraduate Medical Journal, 2002; 78: 63-70
[16] Waaijenborg S, et al. Waning of maternal antibodies against measles, mumps, rubella, and varicella in communities with contrasting vaccination coverage. J Infect Dis. 2013 Jul; 208(1): 10-16
[17] Meadows DH. Thinking in Systems: A Primer. Chelsea Green Publishing, 2008
[18] Heffernan JM, Keeling, MJ. Implications of Vaccination and Waning Immunity. Proc R Soc B, 2009; 276(1664): 2071-2080
[19] Sencer DJ, Dull HD, Langmuir AD, Epidemiologic Basis for Eradication of Measles in 1967, Public Health Reports, 1967: 82(33); 256
(David Vickers, PhD, BIG Media Ltd., 2025)