A recent CDC discussion document claimed that the, “Risk of myocarditis in individuals post-SARS-CoV-2 infection was 6-34 times higher compared to those who received mRNA vaccine.”[1]The “6-34 times” number refers to the risk ratio (or morbidity ratio) of the disease versus the vaccine, and is of great interest, particularly with the expectation of immediate FDA vaccine submissions for children under 5 years old.[2]At such time these vaccines are approved for young children, it would be incumbent on parents to understand where these numbers come from and what the probable risk ratios are for their children.
Myocarditis – or an inflammation of the heart – is a serious disease, of which much has been written during the COVID-19 pandemic. This interest is driven by a causal link of myocarditis to both the COVID virus as a sequela, and to the COVID vaccine as an adverse event following immunization (AEFI), as shown in this article Analysis of severe events following COVID vaccine shows increased incidence of myocarditis and lymphadenopathy. Given that the highest myocarditis AEFI ranges in this work were for the youngest males being vaccinated at the time, parents of younger children may wonder about risk ratios for their kids.
Estimating these ratios is difficult, uncertain, and subject to error. But it is a worthwhile exercise, with a foundation in the rational utility of vaccination, as shown in this article Prisoner’s dilemma and vaccination, where a high ratio increases the value of the vaccine. We shall break down the problem, lay out the challenges, and offer a likely range of the risk ratio for the demographics most at risk of myocarditis.
Why is it so difficult to estimate the rates of myocarditis in this context?
The risk ratio of myocarditis, or the ratio of the chances of developing myocarditis as a result of contracting COVID versus receiving the COVID mRNA vaccine, is difficult to estimate for a variety of reasons, many of them discussed in detail in this article Analysis of severe events following COVID vaccine shows increased incidence of myocarditis and lymphadenopathy.
Those reasons include:
- Various journal investigations have used different study or risk parameters. This is important in comparing events against background rates, as well as between studies.
- Assessment of the myocarditis AEFI is dependent on the quality of the reporting structure in each governmental or health jurisdiction. Passive systems, such as VAERS, are known to have a higher probability of missing an AEFI report than active systems.[3]
- The AEFI analyses have been lumped according to different demographic classifications, making comparisons challenging.
- Myocarditis and pericarditis (inflammation of the pericardium, or sac enclosing the heart) are sometimes – but not always – lumped together.
AEFI vetting analysis is itself subject to an algorithmic procedure, which will not be the same for all studies. That was shown in this article Taking a responsible look at adverse events following immunization.
- COVID-related myocarditis must also be understood in order for the risk ratio to be estimated, and these estimates have their own challenges including unreported COVID cases.[4]
- There have been very few COVID-causal myocarditis studies on young children.[5]
- Different populations may be used for each study, and/or methods of controlling the study, such as creating medical “twins”.
Any of these differences makes assessing the true rates of myocarditis and inferring causation challenging – even potentially invalid – and they make comparing rates of one myocarditis cause to another in a separate study equally questionable.
When experts and journalists – including our team at BIG Media Ltd. – make such comparisons, the reader should be cautious in the level of confidence they assign to the results. Nevertheless, these comparisons and ratios must be estimated as the best current answers until better and more congruous and consistent data is produced.
Our past understanding of myocarditis from COVID and from the vaccine
In this article Analysis of severe events following COVID vaccine shows increased incidence of myocarditis and lymphadenopathy, we examined four large-scale studies evaluating the incidence of AEFIs and disease sequelae both after the Pfizer COVID mRNA vaccine and COVID disease. All of the challenges listed above impacted this comparison, in one way or another. The best results based on experimental design were nevertheless assessed. The results concerning myocarditis are summarized below:
- COVID-causal myocarditis and pericarditis across age groups in the study was significant.
- The estimated risk ratio for COVID-related versus vaccine-related with different cohorts and across adult age groups was: 6.9x for myocarditis and 11x for pericarditis. The authors of the study this was derived from do not create these ratios, though they display the risk differences (against control) for both outcomes.[6]
- AEFI, or vaccine-causal myocarditis, affects men far more than women, and younger men far more than older men. The youngest age group in the study is men in the 16-19 year category.[7]
o The AEFI rate per 100,000 persons for myocarditis across all sexes and age groups was 2.40
o The AEFI rate per 100,000 persons for myocarditis for men aged 16-19 was the highest at 15.58
No AEFI rate for persons younger than the 16-19 was possible at the time of these studies, and none of the studies allowed for stratified, age- and sex-specified risk ratios of COVID-causal versus vaccine-causal myocarditis. The lack of data for younger males leaves parents and other decision makers unable to quantify myocarditis rates attributed to COVID or to the vaccines, for children.
Myocarditis attributed to COVID, with a focus on young people
A preprint study on the rates of myocarditis following COVID infection in younger people has been made available and is being referenced by the CDC.[8][9]The motivation for the work, which was carried out in the United States on persons aged 12-19, was to address questions left unanswered by previous studies. The work was carried out with what appears to be reasonable experimental design, and the estimated COVID-causal myocarditis rates per 100,000 include an adjusted estimate that attempts to account for missed COVID-19 cases.
The rationale for this adjustment is as follows: due to its severity, myocarditis cases are expected to be identified by the health care systems under observation. But a significant number of COVID cases are expected to be missed by the same health care systems, particularly for young people in whom COVID is more often asymptomatic or mild.[10] The estimation of missed COVID cases was performed by referencing other population case rates within the U.S. for the same study period. The adjustment is itself an estimate and subject to error, but likely increases the accuracy of the estimated rates.
The results are shown in the table below and are given per 100,000 persons. Young males and females seem to develop myocarditis as sequelae to COVID in significant numbers. And at higher rates for males than females for most age groups.[11]Surprisingly, the COVID-attributed myocarditis rate for females aged 16-19 is higher than for males in this particular study. The adjusted rates are lower than the measured rates in all cases, and are likely more accurate.
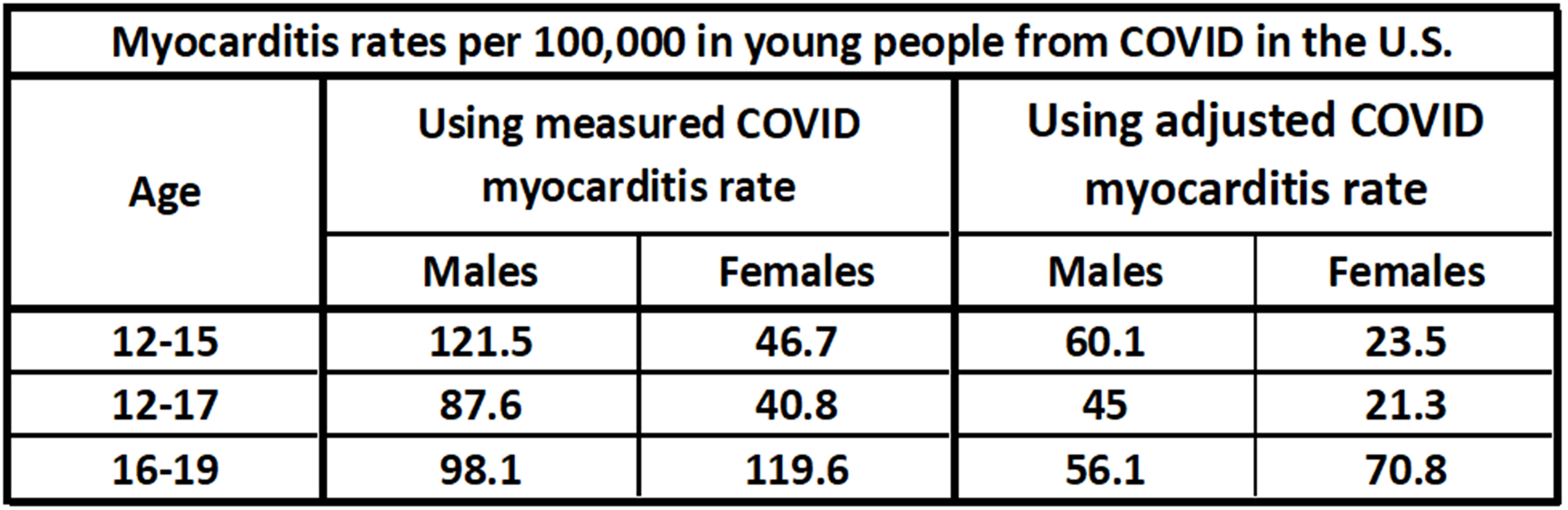
Estimates for COVID-attributed myocarditis rates in young people, per 100,000 persons. Adjusted rates attempt to compensate for missing cases and are likely more accurate than the measured rates.[12]
Myocarditis attributed to the vaccine, with a focus on young people
Although one of the previous studies examined in Analysis of severe events following COVID vaccine shows increased incidence of myocarditis and lymphadenopathy showed a clear, significant dropoff in myocarditis AEFIs from the mRNA vaccines for ages above 16-19 years old, there was no data to show if the rate of vaccine-causal myocarditis drops for ages below 16-19 years.[13]This is a critical consideration for all children’s vaccination and will be important in the upcoming decision of whether or not children aged 0-4 should be vaccinated.
In determining risk ratios for myocarditis attributed to COVID versus the vaccine, having AEFI studies that break down results by age in a detailed, stratified manner would be very useful. There have recently been three studies of the myocarditis AEFI in children that use the U.S. VAERS system, and one that uses data from Denmark. [14][15][16][17]All four studies confirm that the myocarditis AEFI from mRNA COVID vaccines occur in statistically significant, above background, rates in children under 18 years old. The myocarditis AEFI rate from VAERS studies will likely be underestimated due to an under-reporting bias in this passive reporting system.[18][19]Three of the four studies employed large age categories, and were not useful, but one of them used detailed age stratification, and we show those results in the following charts.[20]
The study breaks down results by mRNA vaccine type (Pfizer or Moderna), age group, and sex. Results are given per 100,000 doses, and we use the same range on the vertical axis for each chart so that comparisons can be made visually.
The first chart is for the Pfizer vaccine, and for males. It shows a peak myocarditis AEFI rate in the 16-17-year age category. The 12-15 age group has a lower rate. Year by year case data confirms that the incidence rate drops for each year below 16. This is a key finding and supports suggestions that the myocarditis AEFI is related to male puberty (or testosterone), and may not be as prevalent an issue in children under five years old.[21]These rates are in the range of, but appear somewhat lower than, the active reporting study done previously with a myocarditis AEFI rate of 15.58 per 100,000 for males aged 16-19.
The Pfizer myocarditis AEFI data for males can be combined to give the two-dose AEFI rate for males in the 12-17 range by adding rates, given they are each per 100,000 persons. This combined estimate of 9.54 per 100,000 will be used later.
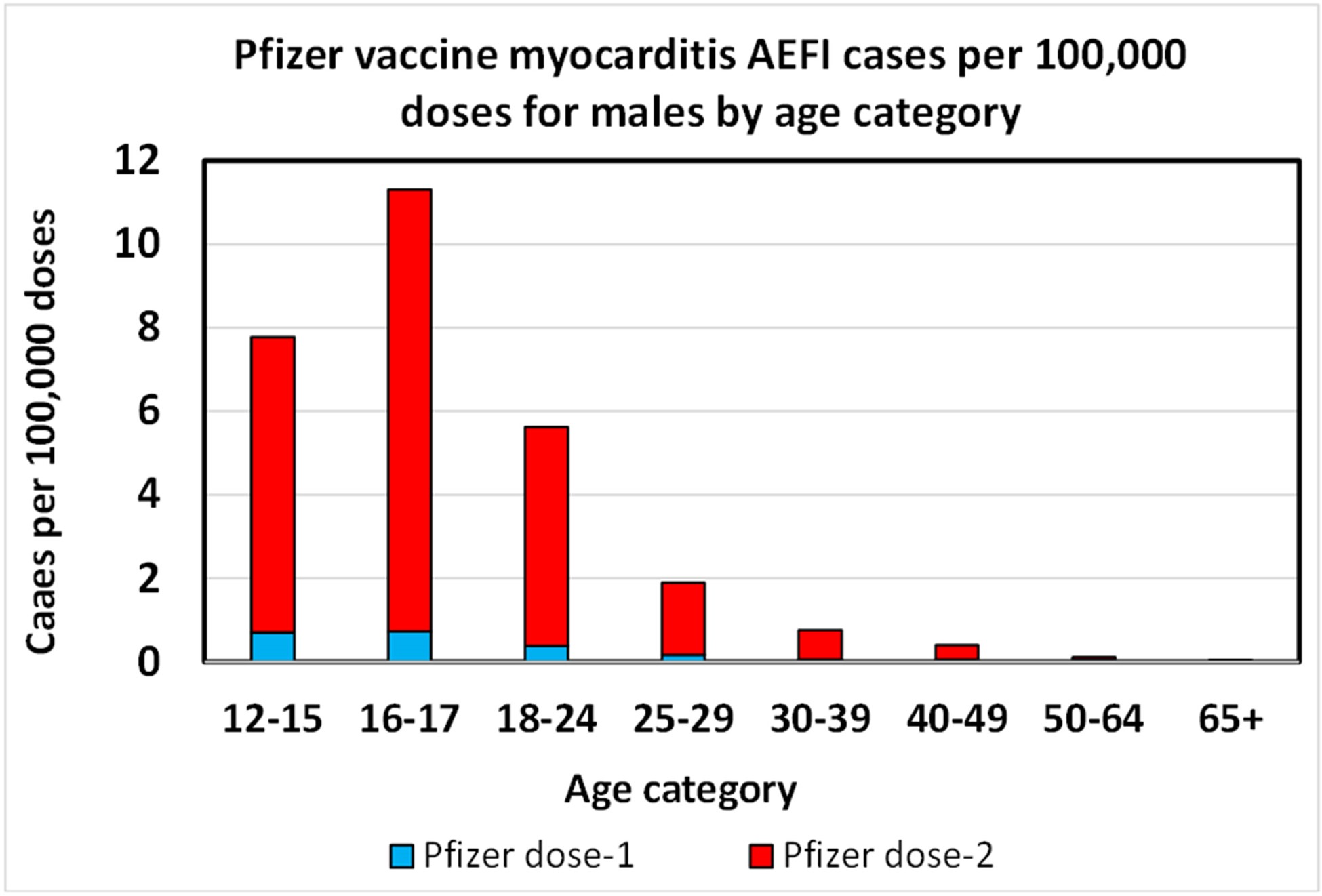
Pfizer myocarditis AEFI rate per 100,000 doses for young males.[22]The dropoff below 16 years old is confirmed by other, per-year data.
The Moderna results for males are similar to the Pfizer results, except that they lack data for categories below 18 years old. The absence of data below the age of 18 makes analysis of risk ratios impossible for the myocarditis vaccine for persons under 18 at this time.
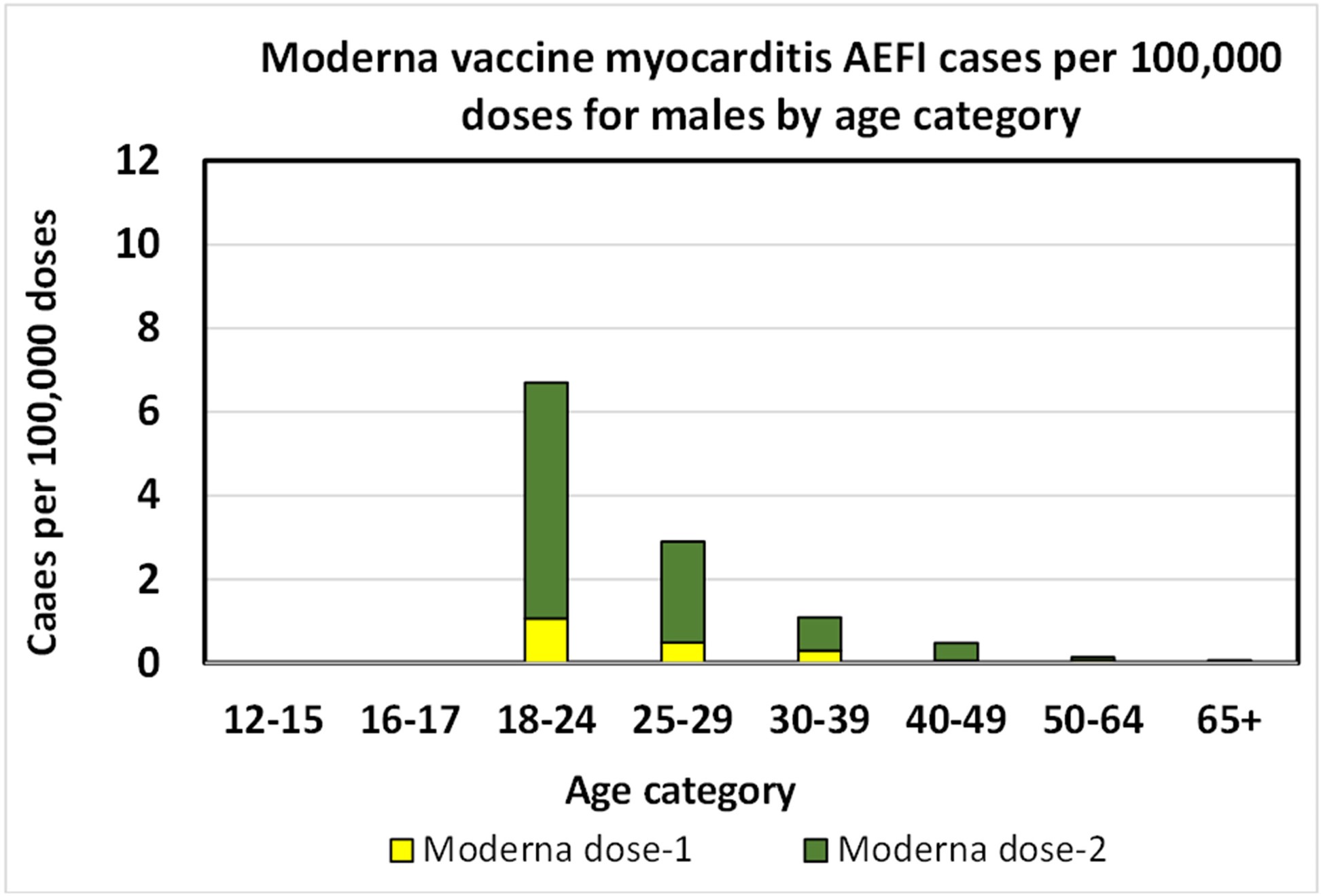
Moderna myocarditis AEFI rate per 100,000 doses for young males.[23]There is not sufficient Moderna data below 18 years of age to chart it.
The Pfizer data for females shows a much lower myocarditis AEFI rate, though the trend – peaking at age 16-17 – is similar.
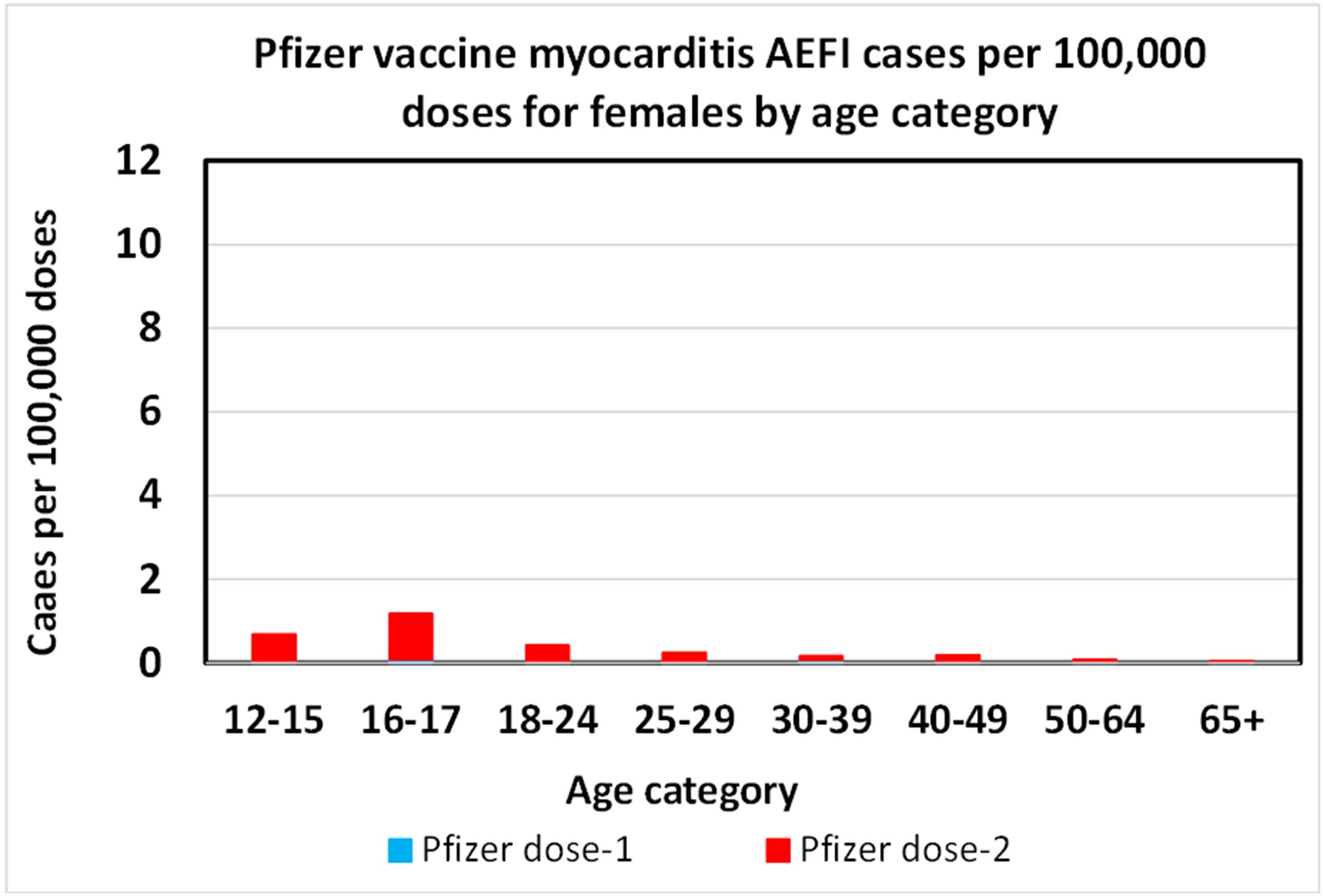
Pfizer myocarditis AEFI rate per 100,000 doses for young females.[24]The drop off below 16 years old is confirmed by other, per-year data.
As it was for the males, the Moderna results for females are similar to the Pfizer results, except that they lack data for categories below 18 years old.
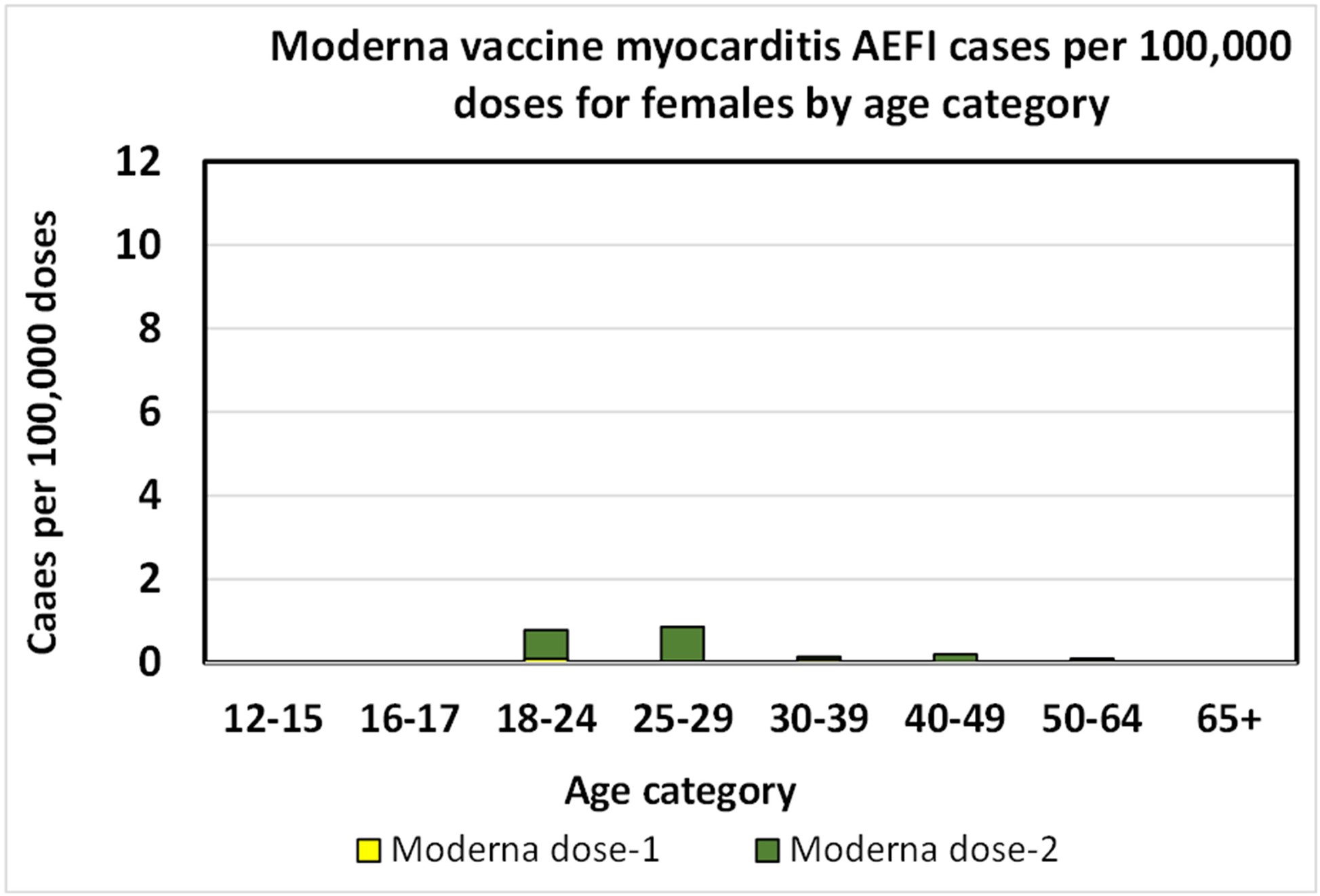
Moderna myocarditis AEFI rate per 100,000 doses for young females.[25]The Moderna data below 18 years of age is insufficient to chart.
Estimate of the myocarditis risk ratio
Any risk ratio of myocarditis attributable to COVID infection versus the COVID vaccine requires a matching of identical demographics and genders across studies. This is not ideal, and results from such an estimate should be viewed cautiously.
From the Pfizer elements of the VAERS study shown directly above, AEFI estimates may be used for the 12-15 and 12-17 age categories. From the Israel study written about here and first discussed in Analysis of severe events following COVID vaccine shows increased incidence of myocarditis and lymphadenopathy, AEFI estimates for the 16-19 category can be used. A summary of this data is shown in the table below, per 100,000 persons assuming a two-dose regimen.
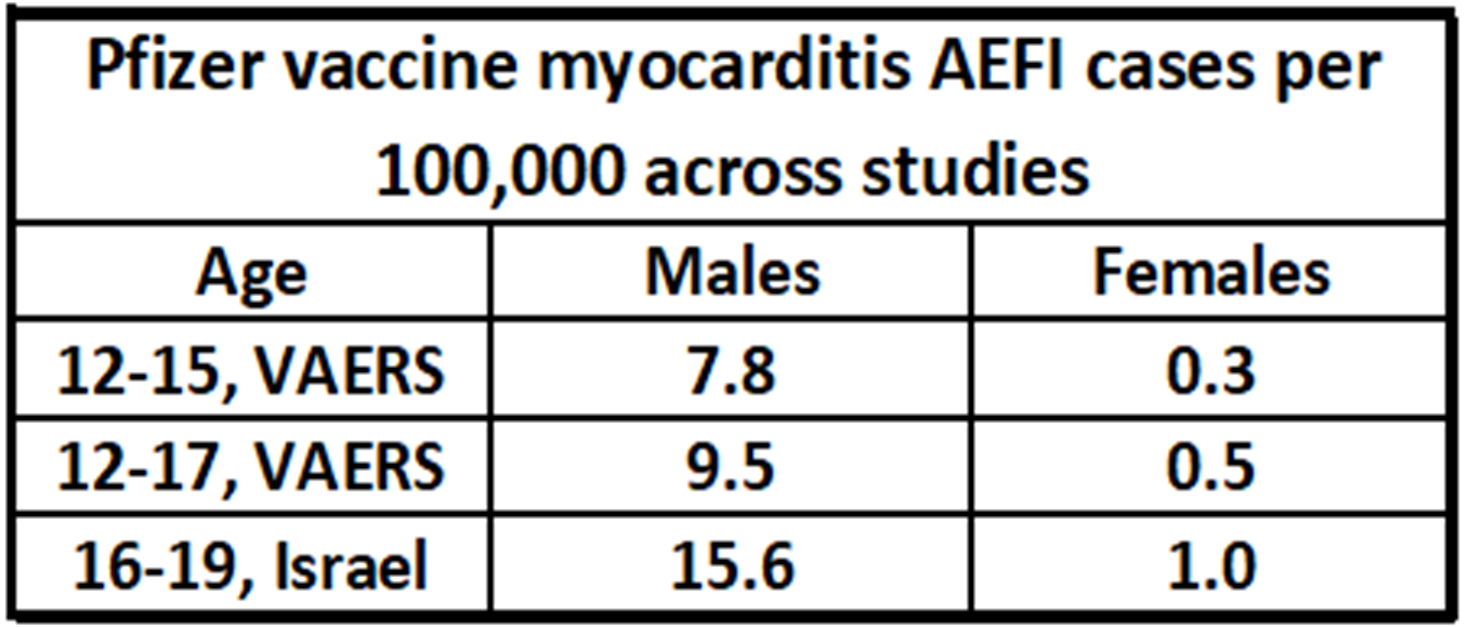
The best estimates of vaccine-attributable (AEFI) myocarditis rates per 100,000 persons taken across studies.[26][27]
And the rates for myocarditis for these same age categories may be taken from the recent U.S. study on young people shown earlier in this article.
The data is combined in the chart below to estimate risk ratios. A low and a high estimate are given through the use of either the measured COVID attributed myocarditis rate or the adjusted rate. It should be noted that the real range of uncertainty is larger than this range. Nevertheless, an estimated range of about 3 to 16 could be taken for young males, and between 45 and 140 for young females in these age categories. These risk ratios will be higher for older persons due to the rapid falloff of AEFI rates by age. It is also expected that the risk ratio will be higher for younger children, considering the AEFI-demographic trend, but this should be shown empirically. Keep in mind that a higher risk ratio signifies that contracting the disease (myocarditis in this case) is less likely from the vaccine, than from a consequence of COVID.
As has been noted, AEFI rates are highly dependent on age and gender, and lumping of age groups and genders would obscure the risk ratio analysis for the at-risk groups.
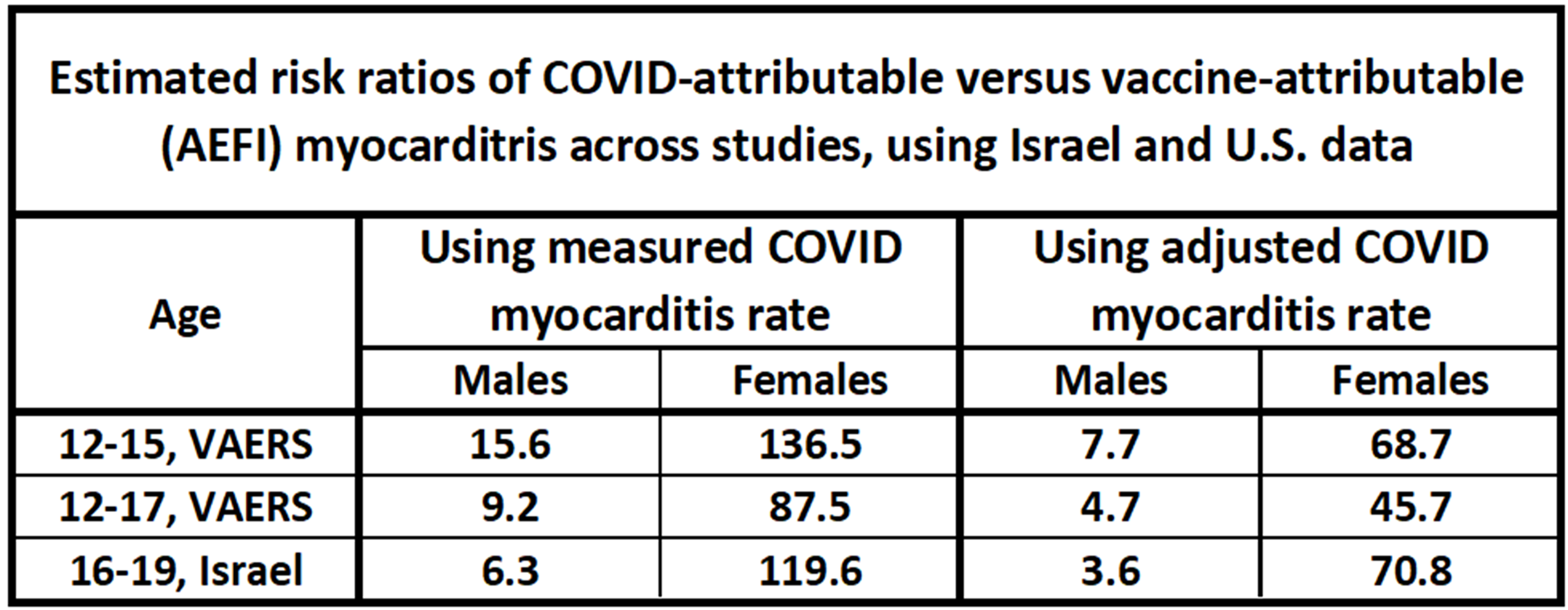
The range of the myocarditis risk ratios for COVID versus the COVID vaccine for young males and females. Risk ratios for older individuals will be much higher. Calculated from [28][29][30].
What does history with other vaccines tell us?
The data above suggests that COVID likely causes far more incidents of myocarditis per population than the mRNA COVID vaccines, even for the most at-risk demographics. Readers may wonder how the lowest risk ratios compare to severe AEFIs from other vaccines. In the article, Analysis of COVID vaccine AEFIs, Part I, it was noted that risk ratios for severe AEFIs were often on the order of 1,000. Many of these severe AEFIs were very serious, such as death from the tetanus shot (risk ratio of >100,000), paralysis from the polio vaccine (risk ratio >1,000) or encephalitis from the measles vaccine (risk ratio of about 1,000).
Although myocarditis is not generally as severe as, say, death, it is concerning. Further, although the risk ratio for myocarditis and COVID rises rapidly from the most at-risk group of 16-year-old males, a ratio on the order of 3 to 16 is historically low for a severe AEFI.
Summary
Estimates of myocarditis in children, whether it is attributable to COVID infection or to the COVID vaccines are difficult to calculate and are highly uncertain. We have nevertheless taken the key findings available to break down a series of ranges for these rates, and the resultant risk ratio of myocarditis sequelae to the disease or following vaccination. Please view these results with some caution, as they will likely be confirmed or improved with additional data in the future. The results:
- Myocarditis that occurs after COVID infection or the COVID vaccine is rare but happens often enough that we can be reasonably confident that it can occur after either the disease or the vaccine.
- There are significant challenges in estimating precisely what the frequency of myocarditis is, from either the virus or vaccine.
- Myocarditis after COVID occurs with greater frequency than with the COVID vaccine, probably by a ratio greater than 3-6 times, even in the most at-risk demographics. This range increases dramatically for demographics with lower risk.
- Males are afflicted by vaccine-attributable myocarditis more often than females.
- Myocarditis (as an AEFI) appears the most in males at age 16-17. This frequency drops off in both older males and in younger males. This suggests, but does not prove, that children under 5 years old are less at risk of vaccine-associated myocarditis than older children.
- When compared to other (historical) severe disease/AEFI risk ratios of other vaccine-preventable diseases, such as polio, the measles, myocarditis (as an AEFI) is low.
References
[1] Rosenblum, Hannah, August 30, 2021, Pfizer-BioNTech COVID-10 vaccine and myocarditis in individuals aged 16-29 years: Benefits-Risk Discussion, CDC
[2] Neergaard, Lauran, March 23, 2022, Moderna Says Its Low-Dose COVID Shots Work for Kids Under 6, NBC
[3] Barda, Noam, et al, 2021, Safety of the BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Setting, New England Journal of Medicine, 385
[4] Singer, Mendel, et al, 2021, Risk of Myocarditis from COVID-19 Infection in People Under Age 20: A Population-Based Analysis, medRxiv, Preprint
[5] Oster, Matthew, et al, January 25, 2022, Myocarditis Cases Reported After mRNA-Based COVID Vaccination in the US From December 2020 to August 2021
[6] Barda, Noam, et al, 2021, Safety of the BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Setting, New England Journal of Medicine, 385
[7] Mevorach, Dror, et al., 2021, Myocarditis after BNT162b2 mRNA Vaccine against Covid-19 in Israel, N. Engl. J. Med.V385, 2140-2149
[8] Rosenblum, Hannah, August 30, 2021, Pfizer-BioNTech COVID-10 vaccine and myocarditis in individuals aged 16-29 years: Benefits-Risk Discussion, CDC
[9] Singer, Mendel, et al, 2021, Risk of Myocarditis from COVID-19 Infection in People Under Age 20: A Population-Based Analysis, medRxiv, Preprint
[10] Singer, Mendel, et al, 2021, Risk of Myocarditis from COVID-19 Infection in People Under Age 20: A Population-Based Analysis, medRxiv, Preprint
[11] Singer, Mendel, et al, 2021, Risk of Myocarditis from COVID-19 Infection in People Under Age 20: A Population-Based Analysis, medRxiv, Preprint
[12] Singer, Mendel, et al, 2021, Risk of Myocarditis from COVID-19 Infection in People Under Age 20: A Population-Based Analysis, medRxiv, Preprint
[13] Mevorach, Dror, et al., 2021, Myocarditis after BNT162b2 mRNA Vaccine against Covid-19 in Israel, N. Engl. J. Med.V385, 2140-2149
[14] Oster, Matthew, et al, January 25, 2022, Myocarditis Cases Reported After mRNA-Based COVID Vaccination in the US From December 2020 to August 2021
[15] Hajjo, Rima, et al, 2021, Shedding the Light on Post-Vaccine Myocarditis and Pericarditis in COVID-19 and Non-COVID-19 Vaccine Recipients, Vaccines 2021, 8, 1186
[16] Hause, Anne, et al, December 31, 2021, COVID-19 Vaccine Safety in Children Aged 5-11 Years—United States, November 3-December 19, 2021 CDC MMWR Vol 70
[17] Husby, Anders, et al, December 16, 2021, BMJ, SARS-CoV-2 vaccination and myocarditis or myopericarditis: population based cohort study, BMJ
[18] Barda, Noam, et al, 2021, Safety of the BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Setting, New England Journal of Medicine, 385
[19] Oster, Matthew, et al, January 25, 2022, Myocarditis Cases Reported After mRNA-Based COVID Vaccination in the US From December 2020 to August 2021
[20] Oster, Matthew, et al, January 25, 2022, Myocarditis Cases Reported After mRNA-Based COVID Vaccination in the US From December 2020 to August 2021
[21] Neergaard, Lauran, March 23, 2022, Moderna Says Its Low-Dose COVID Shots Work for Kids Under 6, NBC
[22] Oster, Matthew, et al, January 25, 2022, Myocarditis Cases Reported After mRNA-Based COVID Vaccination in the US From December 2020 to August 2021
[23] Oster, Matthew, et al, January 25, 2022, Myocarditis Cases Reported After mRNA-Based COVID Vaccination in the US From December 2020 to August 2021
[24] Oster, Matthew, et al, January 25, 2022, Myocarditis Cases Reported After mRNA-Based COVID Vaccination in the US From December 2020 to August 2021
[25] Oster, Matthew, et al, January 25, 2022, Myocarditis Cases Reported After mRNA-Based COVID Vaccination in the US From December 2020 to August 2021
[26] Oster, Matthew, et al, January 25, 2022, Myocarditis Cases Reported After mRNA-Based COVID Vaccination in the US From December 2020 to August 2021
[27] Mevorach, Dror, et al., 2021, Myocarditis after BNT162b2 mRNA Vaccine against Covid-19 in Israel, N. Engl. J. Med.V385, 2140-2149
[28] Singer, Mendel, et al, 2021, Risk of Myocarditis from COVID-19 Infection in People Under Age 20: A Population-Based Analysis, medRxiv, Preprint
[29] Oster, Matthew, et al, January 25, 2022, Myocarditis Cases Reported After mRNA-Based COVID Vaccination in the US From December 2020 to August 2021
[30] Mevorach, Dror, et al., 2021, Myocarditis after BNT162b2 mRNA Vaccine against Covid-19 in Israel, N. Engl. J. Med.V385, 2140-2149
(Lee Hunt – BIG Media Ltd., 2022)